Your CO2 monitor reads 1,200 ppm in your bedroom mid-morning. Is that concerning? The short answer: it indicates marginal ventilation—acceptable by some standards but not optimal.

PuroAir 400 — HEPA 14 Air Purifier
- Covers large rooms up to 2,145 sq ft
- World’s first HEPA 14 filter — removes 99.995% of particles
- Auto air quality sensor · whisper-quiet · free shipping
- 100-day money-back guarantee · trusted by 900,000+ customers
We may earn a small commission if you buy through this link — at no extra cost to you.
ASHRAE’s widely-cited guideline states indoor CO2 should not exceed outdoor air +700 ppm. With outdoor air currently at ~420 ppm, this translates to 1,120 ppm maximum indoors. But this threshold represents a ventilation proxy, not a health limit—research documents cognitive performance declining at concentrations as low as 1,000 ppm, and “sick building syndrome” symptoms appearing above this level. Meanwhile, OSHA’s occupational exposure limit of 5,000 ppm (8-hour average) applies to industrial settings preventing acute CO2 toxicity, not comfort or cognitive function in everyday spaces.
The normal range for well-ventilated indoor spaces is 600-1,000 ppm. Outdoor air measures ~420 ppm currently (rising from 315 ppm in 1960 and 400 ppm in 2015). Good ventilation adds 200-600 ppm from human respiration creating comfortable 600-1,000 ppm steady state. Research confirms spaces achieving 15-20 CFM outdoor air per person (ASHRAE Standard 62.1 recommendation) typically maintain CO2 below 1,000 ppm automatically—making this threshold a useful proxy for adequate ventilation rather than dangerous pollutant concentration itself. The confusion: ASHRAE Standard 62.1 hasn’t contained an actual CO2 limit for 30 years—yet practitioners still cite “1,000 ppm ASHRAE limit” that no longer exists in any current standard.
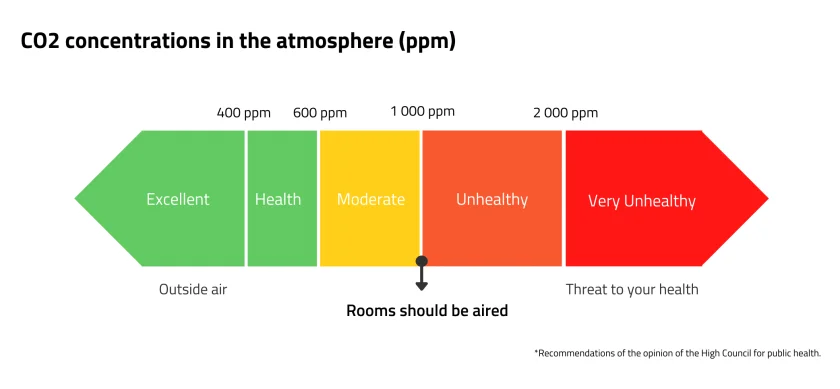
This guide clarifies what different CO2 levels actually mean (600 ppm = excellent ventilation; 1,500 ppm = stuffy air, cognitive decline documented; 2,500 ppm = poor ventilation, symptoms common; 5,000 ppm = occupational safety threshold), explains why bedrooms routinely exceed guidelines overnight (closed doors, high occupancy density, tight construction), and determines when measurement indicates action needed versus normal fluctuation within acceptable range.
Outdoor Baseline: 420 ppm and Rising
Understanding indoor CO2 requires knowing outdoor baseline.

PuroAir 240 — HEPA Air Purifier
- Ideal for bedrooms and rooms up to 240 sq ft
- Captures 99.9% of airborne pollutants including mold spores
- Whisper-quiet sleep mode — won’t disturb your rest
- 100-day money-back guarantee · trusted by 900,000+ customers
We may earn a small commission if you buy through this link — at no extra cost to you.
Current Outdoor Concentration
2025 average: ~420-425 ppm globally (NOAA Mauna Loa Observatory)
Historical context:
- Pre-industrial (before 1800): ~280 ppm
- 1960: 317 ppm
- 2000: 370 ppm
- 2015: 400 ppm (milestone crossed)
- 2025: 420-425 ppm
Annual increase: ~2-3 ppm per year currently—accelerating trend.
Why Outdoor Matters for Indoor
Indoor = Outdoor + Occupant contribution: CO2 indoors starts at outdoor baseline (~420 ppm) then rises based on occupant density, activity, and ventilation rate.
ASHRAE guideline structure: Recommends indoor not exceed outdoor +700 ppm—meaning guideline automatically adjusts as outdoor baseline rises.
Example calculation:
- Outdoor: 420 ppm
- ASHRAE maximum addition: +700 ppm
- Indoor guideline: 420 + 700 = 1,120 ppm
Implication: As outdoor CO2 continues rising, “acceptable” indoor levels rise proportionally unless guidelines change from relative to absolute thresholds.
The ASHRAE Guideline: Outdoor +700 ppm (≈1,100 ppm)
Most commonly cited threshold—but widely misunderstood.
The Actual Guideline
ASHRAE Standard 62.1-2022 guidance: Indoor CO2 concentration should not exceed outdoor air concentration +700 ppm under steady-state conditions.
Typical application: With outdoor at ~420 ppm, this yields 1,120 ppm indoor maximum.
Common simplification: Practitioners often cite “1,000 ppm limit” or “below 1,000 ppm” as rule of thumb—close approximation but technically imprecise.
What This Threshold Represents
Not a direct health limit: Research emphasizes CO2 at concentrations typically found in buildings (1,000-2,000 ppm) “is not a direct health risk” itself.
Ventilation proxy: The +700 ppm threshold indicates outdoor air ventilation rate of approximately 15 CFM per person—the ASHRAE recommended minimum for acceptable IAQ.
Bioeffluent control: At this ventilation rate, studies show “substantial majority of visitors will be satisfied with respect to human bioeffluents (body odor)”—controlling occupant-generated odors, not CO2 toxicity.
The Confusion: 1,000 ppm “Limit”
Research notes “many practitioners and researchers use 1,000 ppmv as criteria for defining good IAQ and cite ASHRAE Standard 62.1 as source”—but “Standard 62.1 has not contained an indoor CO2 limit for almost 30 years.”
Historical context: Standard 62-1981 included 4,500 mg/m³ (~2,500 ppm) CO2 limit—removed in 1989 due to confusion it caused.
Current reality:No ASHRAE standard contains an indoor CO2 concentration limit—only ventilation rate requirements that typically result in <1,000 ppm when followed.
Why ASHRAE Standard 62.1 Doesn’t Actually Contain a CO2 Limit
Correcting the persistent misconception.
The 1989 Removal
Standard 62-1981: Included performance-based “Indoor Air Quality Procedure” with concentration limits for CO2 (4,500 mg/m³ ≈ 2,500 ppm), formaldehyde, ozone, radon, chlordane.
Problem identified: The CO2 limit “caused confusion” because CO2 concentration alone “is not a good indicator of ventilation or IAQ”—other contaminants (VOCs, particles) unrelated to CO2 can create poor IAQ even with low CO2.
1989 revision:CO2 limit removed from standard—replaced with ventilation rate requirements (CFM per person) that indirectly control CO2 via dilution but don’t specify concentration targets.
Reason: Research determined “CO2 is not a critically important contaminant in indoor air” at typical building concentrations—it’s useful as ventilation indicator, not health-based pollutant limit.
What Standard 62.1 Actually Says
Current approach: Specifies outdoor air ventilation rates (CFM per person or CFM per square foot) based on space type.
Example: Offices require 17 CFM per person outdoor air; classrooms 15 CFM per person.
Resulting CO2: Following these ventilation rates typically keeps CO2 below ~1,000-1,200 ppm—but this is consequence, not requirement.
CO2 as diagnostic: Standard recognizes CO2 monitoring as useful diagnostic tool for verifying ventilation system operates properly—not as compliance metric.
The Persistent Myth
Despite removal 30+ years ago, research confirms “many instances in which practitioners and researchers make claims that building has good IAQ because it complies with 1,000 ppmv CO2 limit in the standard”—demonstrating widespread misinformation.
Correct statement: “Ventilation system designed to ASHRAE 62.1 requirements should maintain CO2 below ~1,000-1,100 ppm.”
Incorrect statement: “ASHRAE 62.1 requires CO2 below 1,000 ppm.” (No such requirement exists)
CO2 as Ventilation Proxy: What It Really Indicates
Understanding the indirect relationship.
The Proxy Principle
Direct measurement challenge: Outdoor air ventilation rate (CFM) difficult to measure in existing buildings without sophisticated equipment.
CO2 as surrogate: Since occupants exhale CO2 at predictable rates (~0.3-0.5 L/min per person), indoor CO2 concentration indicates whether ventilation keeps pace with occupancy.
The relationship: Higher CO2 = insufficient outdoor air for current occupancy; Lower CO2 = adequate outdoor air dilution.
What CO2 Doesn’t Indicate
Other pollutants: Research emphasizes “CO2 concentration is not a good indicator of concentration and occupant acceptance of other indoor contaminants, such as VOCs off-gassing from furnishings and building materials.”
Conclusion:“CO2 concentration is not a reliable indicator of overall building air quality.”
Example: Space could have 600 ppm CO2 (excellent ventilation) but high formaldehyde from new furniture—CO2 wouldn’t detect this problem.
Converse: Space could have 1,200 ppm CO2 (marginal ventilation) but low VOCs—CO2 accurately indicates ventilation deficiency but not necessarily unhealthy total IAQ.
The Limitations
Variable occupancy: CO2 only indicates ventilation relative to current occupancy—empty room with 800 ppm doesn’t mean good ventilation (could indicate poor dilution of residual CO2 from earlier occupancy).
Outdoor air quality: If outdoor air itself polluted (high PM2.5, ozone), increasing ventilation (lowering CO2) may worsen indoor air quality by importing outdoor pollutants.
Activity level: Exercise increases CO2 production ~5x versus sedentary—same ventilation rate yields higher steady-state CO2 in gym versus office.
The Normal Range: 600-1,000 ppm in Well-Ventilated Spaces
What “normal” actually means.
Defining Normal
Well-ventilated indoor spaces: 600-1,000 ppm typical range when following ASHRAE ventilation rates.
Lower end (600-700 ppm): Indicates generous ventilation—often seen in:
- Buildings with operable windows frequently opened
- Spaces with high outdoor air delivery (hospitals, laboratories)
- Low-occupancy areas (1-2 people in large room)
Middle range (800-1,000 ppm): Indicates adequate ventilation meeting ASHRAE guidelines—common in:
- Properly designed/operated offices
- Classrooms with functioning HVAC
- Residential living spaces with mechanical ventilation
Upper end (1,000-1,100 ppm): Approaching guideline threshold—acceptable but marginal:
- Offices/classrooms at end of workday
- Restaurants during meal service
- Conference rooms during meetings
Typical Outdoor to Indoor Increase
Rule of thumb: Indoor CO2 200-600 ppm above outdoor in well-ventilated spaces with moderate occupancy.
Calculation basis:
- Adult at rest: ~0.3-0.5 L/min CO2 production
- ASHRAE 62.1 ventilation: 15-20 CFM/person outdoor air
- Steady-state indoor concentration: Outdoor + (production rate / ventilation rate)
Example: 10 people in 1,000 sq ft office
- CO2 production: 10 × 0.4 L/min = 4 L/min = 240 L/hour
- Ventilation: 10 × 17 CFM = 170 CFM = 290 m³/hour
- Concentration increase: 240 L/hr / 290 m³/hr ≈ 830 ppm
- Indoor level: 420 (outdoor) + 830 = 1,250 ppm
Wait—this exceeds guideline! Correct—demonstrating many real-world spaces exceed theoretical calculations due to imperfect mixing, lower actual ventilation rates than design, or higher occupancy than planned.
Below 600 ppm: Excellent Ventilation (Rare Indoors)
The gold standard—uncommon in typical buildings.
When You See <600 ppm
Unoccupied spaces: Recently vacated room with good ventilation—CO2 diluting toward outdoor levels.
Over-ventilated: Spaces with excessive outdoor air delivery (hospitals, clean rooms, laboratories requiring high air changes).
Low occupancy + good ventilation: Large spaces with 1-2 occupants and functioning HVAC.
Windows open: Cross-ventilation creating 5-10+ air changes hourly—rapidly diluting occupant CO2.
The Harvard COGfx Study Implication
Research finding: Harvard Healthy Buildings study suggests keeping CO2 ≤600 ppm may result in significantly improved cognitive function compared to typical 1,000 ppm levels.
Implication: While 1,000 ppm “acceptable” for comfort, 600 ppm represents emerging target for optimizing cognitive performance in knowledge work settings.
Challenge: Achieving <600 ppm requires substantially higher ventilation rates than ASHRAE minimums—typically 25-35 CFM/person versus standard 15-20 CFM—increasing energy costs significantly.
1,000-1,500 ppm: Stale Air, Cognitive Decline Documented
The “acceptable but not optimal” zone.
Subjective Experience
Reported sensations:
- Air feels “stale” or “stuffy”
- Slight drowsiness, difficulty concentrating
- Post-lunch meeting fatigue (exacerbated by elevated CO2)
- Sensation of “needing to step outside for fresh air”
Mechanism: Not primarily CO2 toxicity—but combination of CO2 + bioeffluents + other contaminants accumulating together in under-ventilated space.
Documented Cognitive Effects
Research findings: Studies document “association between CO2 and decreased cognitive performance at concentrations in range of 1,000 ppmv” including:
- Satish et al. 2012: Cognitive decline at 1,000 ppm
- Allen et al. 2016, 2018: Performance decrements
- Lee et al. 2022, Lu et al. 2024: Concentration-dependent impairment
Magnitude: Effects “concentration-dependent”—worsening progressively as CO2 rises from 1,000 → 1,500 ppm.
Controversy: Some studies show effects, others don’t—“inconsistencies require further investigation” per ASHRAE documentation.
Sick Building Syndrome Association
Research notes:“Indoor concentrations greater than 1,000 ppmv have been associated with increases in self-reported, nonspecific symptoms commonly referred to as sick building syndrome (SBS) symptoms.”
SBS symptoms: Headaches, fatigue, eye/throat irritation, difficulty concentrating—constellation appearing in under-ventilated buildings.
Causation unclear: Whether CO2 itself or co-pollutants accumulating alongside CO2 cause symptoms remains debated.
1,500-2,500 ppm: Poor Ventilation, Symptoms Common
The “action needed” zone.
Typical Locations
Bedrooms overnight: Closed doors, 2 occupants sleeping 8 hours—commonly reach 1,500-2,500 ppm by morning in tight construction without mechanical ventilation (documented in previous articles).
Conference rooms: Extended meetings without ventilation breaks—1,500-2,000 ppm typical after 2-3 hours.
Classrooms: Afternoon sessions in poorly ventilated schools—1,500-2,500 ppm common.
Tight homes: Modern construction (<3 ACH50) without mechanical ventilation—1,500-2,000+ ppm overnight.
Health and Performance Impact
Documented effects:
- Headaches, drowsiness more common (MDH; industry summaries)
- Performance drops more clearly (EHP 2012)
- Sleepiness, reduced concentration documented
- Some experience palpitations at upper end of range
Sleep quality: Previous articles documented “1.3-1.8% sleep efficiency reduction at 1,000-1,300 ppm” with further degradation at higher levels.
Ventilation Inadequacy Indicator
Clear signal: Sustained readings 1,500-2,500 ppm indicate insufficient ventilation for current occupancy—action required.
Recommendations:
- Open windows immediately (if outdoor air quality acceptable)
- Reduce occupancy if possible
- Verify HVAC operating properly
- Consider mechanical ventilation upgrade if recurring problem
Above 2,500 ppm: Inadequate Ventilation, Action Required
The “seriously under-ventilated” zone—avoid prolonged exposure.
When This Occurs
Severe under-ventilation: Tight spaces, high occupancy, no mechanical ventilation, windows closed.
Examples:
- Packed conference room, 3-hour meeting, no breaks
- Bedroom with 3+ occupants overnight (children’s room)
- Small apartment, multiple occupants, no ventilation system
- Vehicle interior (can reach 3,000-5,000 ppm in traffic)
Effects at This Level
Research notes:“Sleepiness, reduced concentration; some experience palpitations” common at 2,500-5,000 ppm range.
Symptoms likely include:
- Pronounced drowsiness
- Difficulty concentrating
- Headaches
- Respiratory discomfort for some
- Strong sense of stuffiness, need for fresh air
Not immediately dangerous: Still far below OSHA 8-hour limit (5,000 ppm) and IDLH (40,000 ppm)—but unacceptable for comfort, health, cognitive function.
Immediate Action
Ventilate aggressively: Open windows, doors creating cross-ventilation; evacuate space temporarily while ventilating.
Long-term: Investigate and fix ventilation deficiency—sustained levels >2,500 ppm indicate serious system problems requiring mechanical ventilation installation or HVAC repairs.
OSHA Occupational Limits: 5,000 ppm (8-Hour) and 30,000 ppm (15-Min)
Workplace safety thresholds—NOT comfort or cognitive targets.
The 5,000 ppm 8-Hour TWA
OSHA Permissible Exposure Limit (PEL):5,000 ppm averaged over 8-hour workday (Time-Weighted Average).
Purpose: Prevent acute CO2 toxicity in industrial settings where CO2 may be generated or stored—breweries, welding operations, dry ice handling, etc.
Not comfort standard: This threshold designed for safety, not IAQ or performance—levels cause discomfort and cognitive impairment long before reaching this concentration.
Context:“5,000 ppm is legal limit, not comfort target”—best practice maintains indoor CO2 far below this ceiling for everyday workplaces.

PuroAir HVAC Mega Filter — MERV 13
- Captures dust mites, mold spores and allergens
- MERV 13 + activated carbon — dual filtration
- Designed for optimal airflow · fits any HVAC system
- Free shipping always · easy DIY installation
We may earn a small commission if you buy through this link — at no extra cost to you.
The 30,000 ppm 15-Minute STEL
NIOSH Short-Term Exposure Limit:30,000 ppm for maximum 15 minutes.
Application:“Not appropriate outside controlled industrial settings”—can cause symptoms, represents emergency exposure tolerance, not acceptable routine condition.
Health effects: At this level, respiratory rate increases noticeably, cardiovascular stress, pronounced discomfort.
The 40,000 ppm IDLH Threshold
Immediately Dangerous to Life or Health.
Definition
NIOSH/OSHA IDLH:40,000 ppm (4% CO2)—concentration “immediately dangerous to life or health.”
Meaning: Exposure at this level could cause death or immediate/delayed permanent adverse health effects OR prevent escape from environment.
Mechanism: At 4-10% CO2, asphyxiation risk as CO2 displaces oxygen—also direct CO2 toxicity affecting blood pH (respiratory acidosis).
Real-World Occurrence
Rare in buildings: Achieving 40,000 ppm requires sealed environment with massive CO2 generation or CO2 release (dry ice, industrial leak, fermentation).
Historical incidents: CO2 accumulation in:
- Silos and fermentation tanks (agricultural)
- Wine cellars during fermentation
- Submarines with CO2 scrubber failures
- Confined spaces with dry ice sublimation
Building safety: Modern buildings essentially never reach IDLH absent extraordinary circumstances (massive CO2 leak, sealed space).
Why Bedrooms Routinely Exceed Guidelines
The overnight CO2 accumulation problem.
The Physics
Closed door: Isolates bedroom from rest of house—minimal air exchange with other spaces.
High occupancy density: 2 adults in 150 sq ft bedroom = ~13 sq ft/person versus office 100-200 sq ft/person.
8-hour duration: Long exposure allowing CO2 to accumulate to high steady state.
CO2 generation: 2 sleeping adults produce ~20-25 L/hour CO2 combined.
Typical bedroom volume: 150 sq ft × 8 ft ceiling = 1,200 cubic feet = 34 m³.
Natural Ventilation Inadequacy
Tight construction: Modern bedroom with closed door may achieve only 0.1-0.15 ACH naturally—5-7 m³/hour air exchange.
Dilution calculation:
- CO2 generation: 22 L/hour
- Air exchange: 6 m³/hour
- Concentration increase: 22 L / 6 m³ ≈ 3,700 ppm above outdoor
- Steady-state: 420 + 3,700 = 4,120 ppm
Reality check: Many bedrooms actually measure 1,500-2,500 ppm overnight—indicating slightly better ventilation than worst-case (perhaps 0.2-0.3 ACH from door gaps, envelope leakage) but still far exceeding guidelines.
The Solution
Mechanical ventilation: Continuous low-level ventilation (MVHR, ERV) targeting 0.35+ ACH total maintains bedroom CO2 <1,000 ppm overnight per previous article on airtight homes showing “90% of MVHR bedrooms <1,500 ppm versus 90% of non-MVHR bedrooms >1,500 ppm.”
Interim measures: Open bedroom door, crack window slightly (weather permitting), install transfer grille allowing air circulation.
Typical Indoor Concentrations by Space Type
Real-world measurements by setting.
Outdoor (Baseline)
Global average: 420-425 ppm (2025)
Local variation: Urban areas may measure 450-500 ppm near traffic; rural areas closer to 400-410 ppm.
Residential
Living areas (well-ventilated): 500-800 ppm daytime Living areas (tight, no mechanical): 800-1,200 ppm Bedrooms overnight (mechanical ventilation): 600-1,000 ppm Bedrooms overnight (no mechanical, closed door): 1,500-2,500 ppm Kitchens during cooking: 800-1,500 ppm (combustion appliances add CO2)
Commercial Offices
Well-designed, properly operated: 600-900 ppm Average office buildings: 800-1,200 ppm Conference rooms (during meetings): 1,000-2,000 ppm Poorly ventilated offices: 1,200-1,800 ppm
Educational
Classrooms (good ventilation): 700-1,000 ppm Classrooms (typical): 1,000-1,500 ppm Classrooms (poor ventilation): 1,500-2,500+ ppm afternoon
Healthcare
Patient rooms: 500-700 ppm (high ventilation rates) Waiting areas: 700-1,200 ppm Operating rooms: 400-600 ppm (very high air changes)
Vehicles
Cars (windows up, recirculation): 2,000-5,000 ppm after 30-60 minutes Airplanes: 800-1,200 ppm typical (high air exchange rate)
Cognitive Performance Impact: The 600 ppm vs 1,000 ppm Debate
Emerging science on optimal levels.
The Harvard Healthy Buildings Research
COGfx study findings: Maintaining CO2 ≤600 ppm resulted in significantly improved cognitive function compared to typical 1,000 ppm levels.
Performance domains affected:
- Strategic thinking
- Information usage
- Crisis response
- Initiative
- Basic activity level
Implication: Current “acceptable” thresholds (1,000 ppm) may be suboptimal for cognitive work—higher ventilation rates (~600 ppm) could improve productivity in knowledge economy.
The Cost-Benefit Question
Ventilation energy: Achieving 600 ppm requires 50-70% more outdoor air than achieving 1,000 ppm—significantly increasing HVAC energy consumption.
Productivity benefit: If cognitive improvement translates to measurable productivity gains, energy cost may be justified by enhanced worker output.
Context-dependent: High-value cognitive work (research, strategy, decision-making) may justify 600 ppm target; routine tasks may not require such low levels.
Research Limitations
ASHRAE notes: While some studies show cognitive effects at 1,000 ppm, “other studies did not show any cognitive effects”—“inconsistencies require further investigation.”
Confounding factors: Studies must “address impacts of stress experienced by subjects and exposure to other contaminants (e.g. bioeffluents) in addition to CO2”—separating direct CO2 effects from co-pollutants challenging.
When CO2 Itself Becomes Health Hazard
Direct CO2 toxicity thresholds.
Low-Level Chronic Exposure (1,000-5,000 ppm)
Current understanding: At concentrations “commonly found in buildings, CO2 is not direct health risk” per ASHRAE—effects primarily from co-pollutants accumulating alongside CO2 in under-ventilated spaces.
Exception: Animal studies show “inflammatory changes consistent with neutrophil activation in blood at 2,000-4,000 ppmv and leakage of fluid from blood vessels into brain tissue at 2,000 ppmv”—suggesting possible brain toxicity from pure CO2 at levels previously considered benign.
Implication:“Further research on mechanisms and human response important due to prevalence of indoor concentrations in excess of 1,000 ppmv.”
Acute High-Level Exposure (>5,000 ppm)
5,000-10,000 ppm: Increased respiratory rate, cardiovascular stress, headaches, dizziness common.
10,000-30,000 ppm: Pronounced drowsiness, nausea, vomiting, visual/hearing disturbances possible.
30,000-40,000 ppm: Severe symptoms—rapid breathing, confusion, unconsciousness risk.
>40,000 ppm (IDLH): Immediate danger—asphyxiation risk as CO2 displaces oxygen, rapid loss of consciousness, death possible.
Mechanism of Toxicity
Respiratory acidosis: High CO2 lowers blood pH—affecting enzyme function, cellular metabolism.
Oxygen displacement: At very high concentrations (>10%), CO2 reduces available oxygen percentage creating hypoxia.
Direct CNS effects: CO2 crosses blood-brain barrier affecting neurotransmitter function, cerebral blood flow.
Measuring CO2: NDIR Sensors and Monitor Selection
Choosing accurate measurement tools.
NDIR Technology
Non-Dispersive Infrared (NDIR): Gold standard for CO2 measurement—uses infrared light absorption at specific wavelength (4.26 µm) where CO2 absorbs strongly.
Accuracy: ±30-50 ppm typical for quality NDIR sensors—sufficient for IAQ applications.
Stability: Minimal drift over time—sensors maintain accuracy months to years with proper calibration.
Avoid: Chemical sensors (metal oxide) for CO2—less accurate, significant drift, poor long-term stability.
Monitor Specifications
Measurement range: Minimum 0-5,000 ppm—adequate for all residential/commercial applications. Wider range (0-10,000 ppm) useful for industrial.
Resolution:1 ppm preferred; 10 ppm acceptable.
Update frequency:Every 1-10 seconds—faster updates better for dynamic environments.
Display: Clear numerical readout; color-coded zones (green <1,000 ppm; yellow 1,000-1,500 ppm; red >1,500 ppm) helpful for quick assessment.
Data logging: Desirable feature—records historical data showing overnight peaks, daily patterns.
Recommended Monitors
Aranet4: $200-250—compact, accurate NDIR, excellent battery life, Bluetooth data transfer Airthings View Plus: $280-300—CO2 + PM2.5 + VOC + radon, comprehensive IAQ monitoring CO2Meter Day/Night: $120-150—simple, accurate, affordable option focusing on CO2 only Awair Element: $250-300—multi-parameter IAQ monitor with app integration
Calibration
Factory calibration: Quality monitors pre-calibrated; typically accurate out-of-box.
Outdoor verification: Occasionally take monitor outdoors—should read ~420 ppm confirming calibration accuracy.
Recalibration frequency: Quality NDIR sensors maintain accuracy 1-3 years before recalibration needed; some monitors offer automatic baseline correction.
Actionable Thresholds: When to Ventilate
Practical decision points based on measured CO2.
<600 ppm: No Action Needed
Assessment: Excellent ventilation—rare indoors.
Action: None required; continue current practices.
600-1,000 ppm: Normal, Acceptable
Assessment: Well-ventilated space meeting ASHRAE guidelines.
Action: Maintain current ventilation; monitor for upward trends.
1,000-1,200 ppm: Marginal, Consider Improving
Assessment: Approaching or slightly exceeding guidelines—acceptable but not optimal.
Action:
- Increase ventilation if pursuing cognitive performance optimization
- Monitor for further increases
- Consider mechanical ventilation if recurring
1,200-1,500 ppm: Elevated, Ventilate When Feasible
Assessment: Above guidelines—indicates insufficient ventilation.
Action:
- Open windows if outdoor air quality acceptable
- Verify HVAC operating properly
- Take ventilation breaks in long meetings
- Consider mechanical ventilation upgrade
1,500-2,500 ppm: Poor, Immediate Action
Assessment: Significantly under-ventilated—symptoms likely.
Action:
- Open windows/doors immediately creating cross-ventilation
- Reduce occupancy if possible
- Investigate ventilation system malfunction
- Mechanical ventilation upgrade likely needed
PuroAir 240
HEPA Air Purifier
Best for
Bedrooms, nurseries, small offices
PuroAir 400
HEPA 14 Air Purifier
Best for
Living rooms, mold & allergy sufferers
We may earn a small commission if you buy through these links — at no extra cost to you.
>2,500 ppm: Inadequate, Evacuate and Fix
Assessment: Severely under-ventilated—unacceptable conditions.
Action:
- Evacuate space temporarily
- Ventilate aggressively (all windows/doors open)
- Do not re-occupy until CO2 <1,500 ppm
- Professional HVAC assessment required
Frequently Asked Questions
What is a normal CO2 level indoors?
– 600-1,000 ppm в well-ventilated spaces
– Outdoor baseline ~420 ppm + 200-600 ppm от occupants
– ASHRAE guideline: <1,120 ppm (outdoor +700 ppm)
What CO2 level is too high indoors?
>1,500 ppm indicates poor ventilation, symptoms common
>2,500 ppm inadequate ventilation, immediate action needed
– OSHA workplace limit 5,000 ppm (safety, not comfort)
– Bedrooms routinely hit 1,500-2,500 ppm overnight без mechanical ventilation
Is 1,000 ppm CO2 safe indoors?
– Safe? Yes – far below toxicity thresholds
– Optimal? Debatable – cognitive decline documented at this level
– ASHRAE uses outdoor +700 ppm (~1,120 ppm) as guideline
– Harvard research suggests 600 ppm better for cognitive performance
– No direct health risk at 1,000 ppm, but indicates marginal ventilation
Why is bedroom CO2 so high at night?
– Closed door isolates bedroom from rest of house
– High occupancy density (2 people in 150 sq ft)
– 8-hour duration allows accumulation
– Tight construction (modern homes <3 ACH50) only 0.1-0.15 ACH natural
– Result: 1,500-2,500 ppm typical без mechanical ventilation
– Solution: MVHR keeps 90% bedrooms <1,500 ppm vs 90% >1,500 без MVHR
How do I lower CO2 levels in my house?
– Open windows creating cross-ventilation (quickest)
– Mechanical ventilation (MVHR/ERV) maintaining 0.35+ ACH
– HVAC fresh air intake increasing outdoor air delivery
– Reduce occupancy in small spaces
– Open bedroom doors allowing air circulation overnight
– Target: maintain <1,000 ppm for comfort, <600 ppm for optimal cognitive performance